What are Granulocytes?
Granulocytes are a type of White Blood Cell. Not all White Blood Cells are Granulocytes, but all Granulocytes are white blood cells. There are a few types of Granulocytes -- Neutrophils, Eosinophils, and Basophils. Each cell is involved in different functions throughout the innate immune system. The innate immune system differs from the adaptive immune system in that it already exists "innately", whereas the adaptive immune system involves things like antibodies and antibody mediated responses. This means that the cells in the innate immune system begin the initial first line defense against pathogens and can respond much earlier to a new threat. Granulocytes are aptly named as they contain "granules" that serve cytotoxic (toxic to cells) and antimicrobial purposes.
Neutrophils
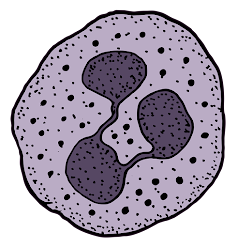 |
| A Neutrophil with visible granules |
Neutrophils are the most abundant Granulocyte in circulation and the most important in regards to infection. They are the recruited to sites of infection by chemical signaling where they have multiple pathways to attempt to defeat an infection. Neutrophils can release cytokines which are inflammatory signaling molecules that can signal other cells of the immune system to report to the site of infection for help. Neutrophils have dozens of different protein granules that they can release to help fight an infection. The granules have different modes of toxicity and ways of damaging the cell of an infectious invader.
Neutrophils can also phagocytize certain microbes. Phagocytosis is the process of ingesting foreign particles, such as an infectious microbe. One ingested, the microbe can be destroyed by processes within the Neutrophil.
Additionally, a function discovered just in the past 20 years of so, Neutrophils also create NETs, or Neutrophil Extracellular Traps. NETs are web like strands consisting mostly of DNA from Neutrophil can also contain granules similar to the granules inside of the Neutrophils cell. The strands can trap microbes and potentially even prevent them from spreading. The granules within the NETs web-matrix act similarly, and have anti-microbial properties.
Eosinophils
Eosinophils are the next most common Granulocyte comprising up to 3% of all circulating granulocytes (in a normal healthy individual). Eosinophils are implicated in certain allergic and asthmatic responses as well as responsible for assisting with defeating parasitic infections, especially intestinal worm type parasites known as Helminths. Many of the common granules in Eosinophils have robust activity against a helminth infection.
Basophils
Basophils are the least common Granulocyte found in circulation -- generally up to 1% in normal healthy individuals. Basophils are also responsible and implicated in allergic reactions and may be responsible for more chronic allergic disease. Basophils release histamine (among other things) in response to certain foreign particles (potentially allergens). Histamine, among many things, dilates the blood vessels, while at the same time making the vessels more permeable. This allows room for other white blood cells and immune mediators to make their way to a site of infection or other unwanted particles. Increased permeability of the vessels allows the cells to make their way to the sites easier. Basophils may also have activity that proves to be anti-parasitic and/or antimicrobial as well.
Granulocytes and Neutropenia
The transfusion of Granulocytes focuses mainly on Neutrophils. When a patient is neutropenic, they are said to have a deficiency in circulating neutrophils called...neutropenia. Neutropenia can be caused by many things such as
Cancers - any cancer affecting the bone marrow could lead to neutropenia depending on its damaging effects on the bone marrow
Chemotherapy -- A common reason for neutropenia is chemotherapeutic agents. Chemotherapy, especially ones designed to help with blood cancers, can cause a suppression of the bone marrow. Since white blood cells are made in the bone marrow, there is a significant loss of production of these cells.
Autoimmune - some patients may have autoantibodies that attack and remove neutrophils from circulation.
Drugs -- certain drugs can cause neutropenia
Sepsis and Infections -- Even infections themselves can cause neutropenia. Neutrophils can be both used up while trying to fight infections and also experience increased destruction and decreased production due to bone marrow suppression in septic events.
Stem Cell Transplant / Immunosuppressants -- Being on immunosuppressants especially after transplants such as Stem Cell Transplants may see neutropenia. Immunosuppressant drugs are essential for ensuring Transplantation Graft rejection does not take hold.
Congenital Neutropenia -- Neutropenia can result from genetic defects that cause neutrophils to be made in lesser amounts or defects that cause neutrophils to be created that lack normal functioning.
Granulocyte Transfusion Process
When a patient is severely neutropenic, they are at risk for severe infection. Without circulating neutrophils, it is rather difficult for the body to fight off infections. A patient would not be transfused granulocytes simply for being neutropenic. A patient that is neutropenic with severe infection should be given antimicrobial (antibiotics/anti-fungals/etc) therapy first. Some patients may also be given drugs that can help stimulate the production of more granulocytes within the body.
It is only when these first line therapies fail, and severe infection is threatening the life of the patient, that granulocyte transfusion is typically considered. Granulocyte transfusions are the one and only time we actually WANT White Blood Cells in our blood products. However, granulocytes MUST be
irradiated to deactivate any T-cell lymphocytes (another type of white blood cell). Without irradiating, the T cells may activate and attack the recipients cells causing severe Transfusion Associated Graft-vs-Host disease.
The efficacy of granulocyte transfusion is debatable in the medical and Transfusion Medicine community. Some studies have shown them to be ineffective at clearing infection (although one major study lacked participants and could not come to the conclusion that it was truly ineffective as a result). Some studies have shown them to be effective. There are many anecdotal reports of physicians seeing an improvement in clinical course after receiving granulocyte transfusions. It is up to the patient's physician as well as a Transfusion Medicine physician to determine if the product is right for the patient's clinical picture.
Prepping Granulocyte Donor
If granulocyte transfusion is agreed upon, the transfusion center will contact their appointed Blood Center to begin looking for donors to recruit. Due to collection techniques, a small amount of Red Blood Cells are generally present in granulocyte units, thus donors should if at all possible be properly ABO/Rh (Blood Type) matched. In the US, when a donor is recruited, they may give the donor G-CSF (Granulocyte-Colony Stimulating Factor). This will cause the donor's body to produce more granulocytes, thus maximizing the amount of granulocytes that can be harvested.
Granulocyte Collection
Once ready to donate, the granulocytes are generally collected via apheresis (a machine that takes in a donors blood, centrifuges it into parts, and removes only what is being collected, and returns the rest into the patient's bloodstream). Once collected, the granulocyte unit must find its way to the patient as soon as possible. Granulocytes have a very short window of use, generally only 24 hours post collection. It is essential that this process is communicated to the patient's clinical team so that once the unit arrives at the Transfusion Center it can be transfused as soon as possible. Patients will typically receive a "course" of granulocyte transfusions, and on average receive a 5-day course. The recruited donor is expected to show up each day to donate for this cause.
Granulocyte Safety Factors to Consider
The physician must also be aware that the vast majority of the time, infectious disease testing will not be completed by the time it is necessary to transfuse the unit. Testing generally takes longer than what the 24-hour expiration time of the unit affords. The physician will usually need to sign off agreeing to this prior to transfusion. The Blood Center will be able to provide infectious disease testing results at a later date if needed as they are still performed, just not completed in time. Blood Centers will typically have other means of ensuring safety in these situations, such as recruiting donors that are known to the Blood Center to have a clean infectious disease background.
Patients must be closely monitored during and after transfusion of granulocytes, as it is not uncommon to have varying degrees of transfusion reactions from a granulocyte transfusion.